
Let’s be honest. Most men were never really taught how female pleasure works. What little we absorbed came from films, locker room conversations, or — let’s face it — pornography, none of which are particularly reliable guides to what actually feels good for a real woman in a real relationship.
If you’re reading this, you’re already doing something most men don’t: actively seeking to understand your partner’s experience. That matters. And it’s exactly where a more satisfying intimate life begins.
This article is a practical guide — grounded in anatomy and backed by current research — to understanding the female body, what tends to feel good and why, and what options exist when physical or hormonal barriers get in the way of pleasure.
Why “Trying Harder” Often Doesn’t Work
Before we get into anatomy, it’s worth addressing something that quietly frustrates a lot of couples: the assumption that more effort automatically produces better results.
Female pleasure is less about technique and more about context, trust, and knowing where to focus attention. A woman’s experience of arousal is highly individual — what one partner loves, another may find uncomfortable or simply neutral. That’s not a problem to be solved with a different move. It’s an invitation to communicate, explore, and stay curious together.
Think of what follows not as a checklist, but as a starting point for that conversation.
Understanding the Key Pleasure Zones
The Clitoris — The Most Reliable Route to Pleasure
If there is one thing research makes unmistakably clear, it is this: the clitoris is central to female sexual pleasure. Studies consistently show that more than 90% of women experience orgasm through clitoral stimulation — yet it remains one of the most overlooked areas in sexual encounters.
What many people don’t realise is that the clitoris is far larger than the small external nub that’s visible. It’s actually an internal structure extending several centimetres inside the body, with two “arms” that run alongside the vaginal walls. This is why certain internal positions and pressures can indirectly stimulate the clitoris even without direct external contact.
The external part of the clitoris — the glans — is extraordinarily sensitive, containing approximately 8,000 nerve endings in a very small area. Many women find direct, sustained pressure uncomfortable; what tends to work better is indirect stimulation, circling around it, varying pressure, and paying close attention to your partner’s responses.
The key takeaway: Don’t skip the clitoris, and don’t rush past it.
The G-Spot — Real, but Highly Individual
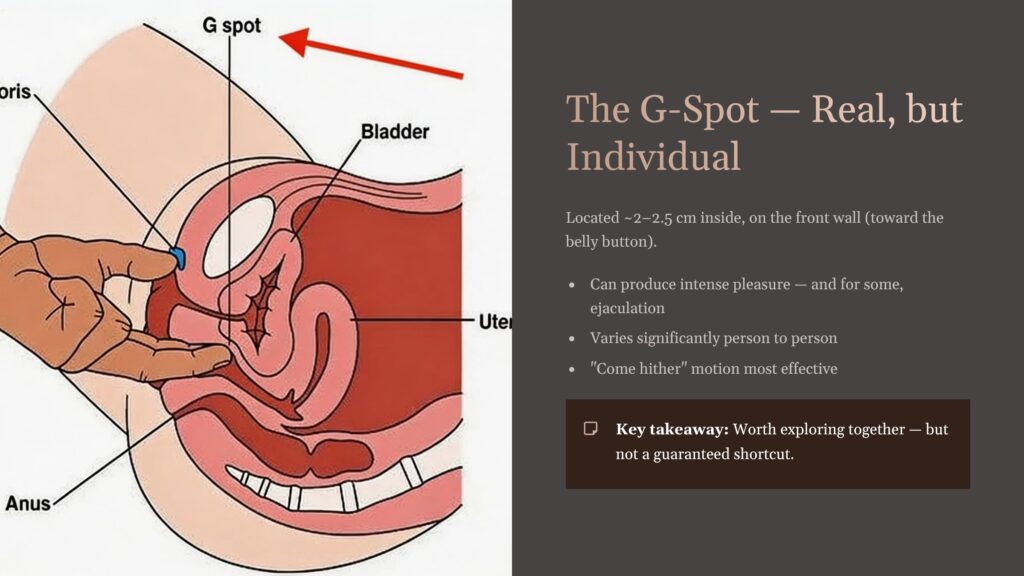
The G-spot is located approximately 2 to 2.5 centimetres inside the vaginal opening, on the front wall — the side facing the belly button. It sits near the urethra and bladder neck, and when stimulated, it can produce intense pleasure for many women, and for some, lead to female ejaculation.
Medical consensus has increasingly moved toward recognising the G-spot as a real anatomical structure, though its prominence varies significantly from person to person. For some women it’s an intensely sensitive area; for others, stimulation there feels like little more than mild pressure.
To explore this area, a “come hither” motion with one or two fingers — gently pressing and stroking the front wall — is the most commonly effective approach. Some positions during intercourse also naturally direct contact toward this area.
The key takeaway: Worth exploring together, but don’t treat it as a guaranteed shortcut. It varies enormously between individuals.
The A-Spot and C-Spot — Deeper Sensitivity
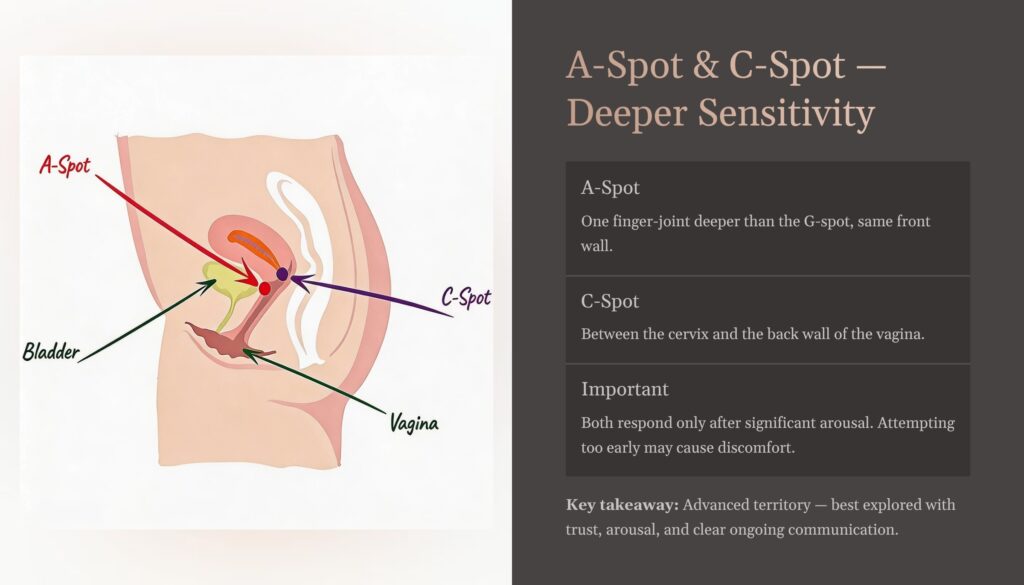
These terms don’t appear in standard medical textbooks, but they’re used increasingly to describe two areas deeper within the vagina that some women find highly pleasurable.
The A-spot sits approximately one finger-joint deeper than the G-spot, on the same front wall. The C-spot is located between the cervix and the back wall of the vagina. Both areas tend to respond better after significant arousal has already built — attempting to stimulate them too early, before the vagina has naturally expanded and lubricated, is unlikely to be pleasurable and may cause discomfort.
The key takeaway: These are advanced territory, best explored after trust and arousal are well established — and only ever with clear, ongoing communication.
Other Sensitive Areas Often Overlooked
The labia minora — the inner folds of the vulva — contain nerve endings similar to those in the clitoris, and gentle attention here can be deeply pleasurable for many women. The area around the vaginal entrance is similarly sensitive.
Some women also find the posterior vaginal wall — the back wall, the side facing away from the belly — more responsive than the front. This is less commonly discussed, but worth exploring if the front wall doesn’t produce the response you both expected.
The key takeaway: The vulva and vaginal entrance deserve far more attention than they typically receive. Slow down here.
When Things Aren’t Working — Understanding Sexual Dysfunction
Sexual difficulties are more common than most couples realise, and far more treatable than many assume. Understanding what’s actually happening — physiologically — is the first step toward addressing it constructively, without blame and without shame.
Researchers typically describe sexual dysfunction in three broad categories:
Desire Disorder is characterised by a persistent lack of sexual interest. It’s particularly common in women who have never experienced orgasm — because if sex hasn’t reliably produced pleasure, the brain has little incentive to seek it out. Addressing the physical barriers to orgasm often resolves the desire issue simultaneously.
Arousal Disorder tends to emerge in longer-term relationships, where routine and familiarity have gradually replaced novelty and anticipation. The body is capable of responding, but the conditions — emotional connection, novelty, context — are no longer reliably present. Improving the quality of the relationship and introducing intentional variety can make a significant difference here.
Orgasmic Disorder involves consistent difficulty reaching climax, and tends to have more complex underlying causes — including hormonal factors, nerve sensitivity, physical structure, and psychological elements. This category often benefits most from professional support.
Medical Options Worth Knowing About
For couples where physical or structural factors are contributing to sexual dissatisfaction, a growing range of medical treatments is available in Australia. These are worth discussing with a qualified medical practitioner — specifically a gynaecologist or sexual health physician — rather than pursuing independently.
Clitoral Hood Reduction: In some women, an enlarged clitoral hood (prepuce) partially covers the external clitoris, limiting sensitivity and making stimulation more difficult. A minor surgical procedure can reduce the hood, increasing direct access and often significantly improving sensitivity. This is a well-established, relatively straightforward procedure.
G-Spot Enhancement: Some clinics offer procedures to augment the G-spot using collagen injections, making the area more prominent and easier to stimulate. Related treatments — sometimes called O-shots — use growth factors derived from the patient’s own blood (PRP), or regenerative agents such as PDRN or stem cells, to enhance nerve sensitivity in the vaginal area. Results and experiences vary; a thorough consultation with a sexual health specialist is essential before pursuing any of these.
Pelvic Floor and Laser Therapy: Vaginal muscle tone plays a significant role in both arousal and orgasm. Muscles that are too tight can cause discomfort and restrict sensation; muscles that are too weak may reduce the intensity of orgasm. Pelvic floor physiotherapy, and in some cases laser treatments, can address both issues — relaxing overactive muscles and strengthening underactive ones. This is particularly relevant for women post-childbirth or in perimenopause.
Sympathetic Nervous System Activation: Research suggests that actively engaging the pelvic floor muscles during intercourse — consciously contracting and releasing the vaginal muscles — can elevate sympathetic nervous system activity, helping the body build toward climax more effectively. This is something couples can explore together without any medical intervention.
The Most Important Thing You Can Do
More than any technique, any zone, or any medical option — the single most effective thing a couple can do to improve their intimate life is talk honestly about what feels good.
This doesn’t have to be a formal or serious conversation. It can happen in the moment, simply and lightly: “Does this feel good? More like this, or less?” Over time, those small, ongoing conversations build a map — unique to your relationship — that no article or textbook can provide.
The expert insight underlying all of this research is simple: the path to a more satisfying physical relationship begins with finding your own erogenous zones, communicating openly with your partner, and seeking professional guidance if physical or hormonal barriers are getting in the way.
You don’t need to be perfect at this. You just need to be curious, attentive, and willing to keep learning together.
This article is intended for educational purposes and does not constitute medical advice. For personalised guidance on sexual health or dysfunction, please consult a qualified medical professional or sexual health specialist.